Histiocytosis, the one word that all Bernese Mountain dog owners dread to hear. But it's not unique to Berners, and not all varieties are fatal. All breeds get histiocytomas, which appear and progress more like a wart. Collies and Shelties get cutaneous histiocytosis which is a nuisance, but not at all deadly. Flat-Coated retrievers get a different form of histiocytic sarcoma. When caught early and surgically removed the progression may be delayed, but this is generally a fatal form of the cancer. Rottweilers, Doberman Pinschers, Golden Retrievers and Labrador Retrievers have all been infrequently diagnosed with malignant histiocytosis, which is always a death sentence. In Bernese, we have both systemic histiocytosis and histiocytic sarcoma. So what is histiocytosis?
First we need to define some of the terms and concepts. The bone marrow produces leukocytes, red blood cells, and platelets. The leukocytes are the white blood cells and they are comprised of three different groups. One of those groups, the nongranulocytes, consists of lymphocytes and monocytes. The monocyte is a phagocytic cell (a cell that ingests other cells or foreign material) which circulates in the blood, but which can develop into either macrophages or dendritic cells when it migrates into body tissue. These are the histiocytes. The histiocytes are an important part of the immune system; the dendritic cells recognize foreign material - antigens - and help stimulate the immune system response to the antigens by presenting them to the T cells. The macrophage cells also help stimulate immune system response as well as devouring foreign material. Histiocytes are found throughout the body in the dermis (the middle and thickest layer of skin) and in the connective tissue. Sarcoma is the name given to cancer of the bone, cartilage, fat, muscle, blood vessels or other connective or supportive tissue. A lesion is an area of abnormal tissue change.
There are two benign forms of histiocytic disease, the histiocytoma and cutaneous histiocytosis. Hystiocytomas are wart-like growths that occur singly on the surface of the skin and usually go away on their own in just a few weeks. Cutaneous histiocytosis occurs as single or multiple skin growths. They may go away on their own, or wax and wane, and may need treatment with corticosteroids or in some more extreme cases require more aggressive immunosuppressive therapy.
Systemic histiocytosis was first described as being separate and distinct from histiocytic sarcoma; later it was defined as a variation of histiocytic sarcoma; and most recently it is back to being considered a separate and distinct form of histiocytosis. The initial presentation of systemic histiocytosis is multiple masses in the skin. These may be found all over in a variety of locations on the body - in the eyelids, on the muzzle, the scrotum - typically the masses are located on the head and extremities rather than the trunk of the body. These masses may be smooth, haired, crusted, or ulcerated. The disease can go into remission on its own, but each recurrent episode generally becomes progressively worse. Eventually it may spread to the spleen, liver, bone marrow and/or lungs, and the disease process mimics that of histiocytic sarcoma. Systemic histiocytosis has been successfully treated with immuno-suppressive drugs, such as Cyclosporin A and Leflunomide, and variable success with immuno-suppressive doses of corticosteroids. I have heard of two cases in which survival exceeded five years from time of diagnosis, and have seen documentation of two cases of survival for over one year, and another documented case of survival for four years. This form of the disease is more frequently seen in males, and has a mean age of 4 years at onset.
Histiocytic sarcoma has several distinct variations: localized, disseminated, and hemophagocytic. Localized histiocytic sarcoma occurs as a localized lesion in a joint, the spleen, lymph nodes, lung, bone marrow or skin. It may take time to spread, but once it does it acts much more like disseminated histiocytic sarcoma.
Disseminated histiocytic sarcoma is a very aggressive form of cancer that is usually already widespread before any symptoms are noted. Symptoms usually include loss of appetite (anorexia), weight loss, lethargy, weakness, and poor general condition. There could be difficulty breathing, coughing, shortness of breath, or abnormal lung sounds. Radiographs may show single or multiple tumors in the lungs, or enlargement of the spleen or liver (splenomegaly or hepatomegaly). The lymph nodes may be enlarged. Blood chemistry may be normal; it may show anemia; it may show a decrease in the number of platelets (thrombocytopenia); or it may show high liver enzyme activity. This cancer affects the spleen, lymph nodes, lungs, and/or bone marrow, but can also affect the liver, central nervous system, kidneys, skeletal muscle, stomach, and adrenal glands.
In cases where the spleen was the primary tumor site and it was detected early, removal of the spleen (splenectomy) has proven beneficial. Severe anemia may be the result of the tumor(s) in the spleen, and once it is removed, the red cell count may return to normal. But disseminated histiocytic sarcoma is a disease that attacks many organs simultaneously, or that metastasizes rapidly, so the dog eventually succumbs from the involvement of the other organs. [Note: in one very notable instance, emergency surgery to remove a corncob allowed early detection of the enlarged spleen, which was also removed. The tumor was histiocytic, and the dog lived an additional three years!] Normally a histiocyte would not destroy red blood cells unless those red cells are abnormal (in which case a Coombs test might be positive - a test used to determine the presence of nonagglutinating antibodies on cells). However, if the histiocytes are activated or have become cancerous, they may display hemophagic syndrome, aggressively destroying normal red blood cells - which would give the appearance of hemolytic anemia.
Disseminated histiocytic sarcoma is generally so far spread throughout the organs at the time of diagnosis as to preclude surgical excision as a viable treatment option. Chemotherapy is used in many cases, but dogs have died soon after starting chemo, or lived for many months without any treatment at all. Survival from time of diagnosis may vary from hours, days, perhaps weeks, and very rarely months. The mean age at onset is 7 years.
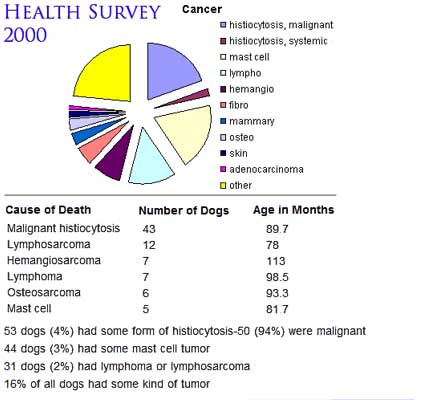
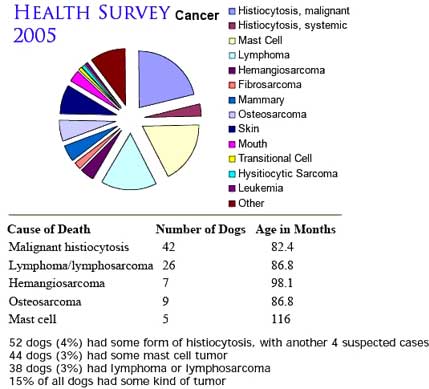
Recent results from the breed health surveys completed in 2000 & 2005, show a significant number of Bernese affected by histiocytic diseases.
2000 & 2005 BMD Health studies Cancer
Studying Histiocytosis
The genetic aspects of MH were evaluated using data stored in the Berner-Garde database in a study initiated in 1989. Out of the 500 tumors collected at that time for the GDC tumor registry, 25.4% of them were histiocytic. The study determined that the general population of Bernese Mountain dogs had a 1 in 20 chance of acquiring a histiocytic disease, but this increased to 1 in 4.5 if either parent had a histiocytic disease. The conclusion of the study was that it is inherited, it is polygenetic, and the heritability factor was calculated to be 0.298.
Researchers continue to study this disease.
Recommendations
This all means that it should be theoretically possible to breed away from histiocytic disease in the breed. But that will require a great deal of work and input from all of us.
Verification and accurate diagnosis of histiocytic disease is imperative. "I think my dog died of histio" or "my vet said it was histio" is an insufficient basis for making accurate diagnoses. Biopsy or necropsy with accurate and hopefully consistent pathology determination is critical.
Sharing the information received from accurate diagnosis is required. Entering the results into open databases like Berner-Garde are necessary to allow breeders to make informed breeding decisions.
Educating the owners to acquire and share accurate diagnoses is an ongoing process.
Understanding and using the data is a time consuming and difficult task and the rewards from this process are not always easy to determine.
As people who love the breed, it is incumbent on us all to help find ways to reduce the incidence of histiocytic disease in our breed. Right now, education and knowledge are the only weapons we have, and they frequently seem dreadfully inadequate. Perhaps some day we will have genetic testing to help us eliminate histiocytic disease from the Bernese Mountain Dog, and we are well positioned to help advance that goal. The existence of the Berner-Garde database, and the BG/MI State DNA/tissue repository is an excellent start. This breed has always had very committed admirers, and they have given us an excellent basis for future progress. We need to share the knowledge that research provides us as a tool improve the health and longevity of our breed.
References:
Affolter, Moore. Canine Histiocytic Proliferative Disease. Annual meeting of the AAVD/ACVD in Maui, Hawaii, 1999.
Brown, Thrall, Getzy, Weiser, Ogilvie. Cytology of Canine Malignant Histiocytosis. Vet Pathol Vol (1986); 23:118-122.
Carioto. Malignant Histiocytosis in a Bernese Mountain Dog Presenting as a Mandibular Mass. Can Vet J (1997); 38:105-107.
Moore. Systemic Histiocytosis of Bernese Mountain Dogs. Vet Pathol (1984); 21:554-563.
Moore, Rosin. Malignant Histiocytosis of Bernese Mountain Dogs. Vet Pathol (1986); 23:1-10.
Padgett, Madewell, Keller, Jodar, Packard. Inheritance of Histiocytosis in Bernese Mountain Dogs. Journal of Small Animal Practice (1995); 36:93-98.
Paterson, Boydell, Pike. Systemic Histiocytosis in the Bernese Mountain Dog. Journal of Small Animal Practice (1995); 36:233-236.
Ramsey, McKay, Rudorf, Dobson. Malignant Histiocytosis in Three Bernese Mountain Dogs. Vet Record (1996); 138:440-444.
Rosin, Moore, Dubielzig. Malignant Histiocytosis in Bernese Mountain Dogs. JAVMA (1986); 188:1041-1045.
Scherlie, Smedes, Feltz, Dougherty, Riis. Ocular Manifestation of Systemic Histiocytosis in a Dog. JAVMA (1992); 201:1229-1232.
Wilkinson, Susan. Histiocytosis in Bernese Mountain Dogs. Paper for Veterinary Medical Genetics class, 1997.
Personal Experiences with Histiocytic diseases in Bernese Mountain Dogs From the Berner-L Mailing List
Histiocytoma
Andrea Madeley � Aari, 6/28/95 � still bouncy and happy in August of 2001!
In December 2000 I was grooming Aari, our 5 year old Berner boy, when I noticed a lump on the inside of his hock. It was about 1/2" diameter and had like this crusty centre. It was red in the middle and looked quite ugly. The vet took a sample from the lump and went to the back room and had a look at it. He was able to rule out mast cell tumour right away. That was good news. Regardless however, there were abnormal cells (not necessarily cancerous) present and with that we decided to remove it anyway and have it analysed. The lab report finding was "Histiocytoma". That's good because that's a benign lump - not that uncommon. But my vote is to get them aspirated / biopsied or removed.
Cutaneous Histiocytosis
No cases submitted for this article; however; 5 cases are reported in the Berner-Garde database as of April, 2009.
Systemic Histiocytosis
Carol Lingley � Arrow, 2/14/97 � 12/8/98
We were unable to get a diagnosis for 22 month old Arrow's eye problems until long after his death. His first noted symptom was squinting in the light, and we were shocked to discover that one eye had so much corneal edema that the retina was detatching. The ophthalmologists guessed it was systemic histiocytosis because he was a BMD, but initial biopsies were negative. Two weeks after his initial vet visit, Arrow had to be euthanized � his lungs were so completely involved that he was suffocating. Four different pathology labs were unable to make any conclusive determination until we finally got the slides sent to UC Davis. Dr. Affolter's comment was that the eye was a "beautiful specimen of systemic histiocytosis."
Ruth Reynolds � Stoney, 11/85 � 8/87
In 1987 Pioneer's Stoneybrook v Arak was diagnosed at the University of Florida vet school with systemic histiocytosis. I reported this to Barbara Packard who put me in touch with Dr. Peter Moore at UCDavis. Dr. Moore told me Stoney was the 8th reported case of histiocytosis in our breed. She was about 15 months old when diagnosed. She had symptoms for at least 6 months.
Stoney's symptoms began with conjunctivitis with initially responded marginally to triple antibiotic plus hydrocortisone ointment. Eventually that treatment lost its effect and her conjunctivitis became very, very bad, such as I have never seen in any dog in my 20 years of working in various vet practices.
Stoney developed bumps in the skin which I describe as similar to the fatpad on one's thumb. They varied in size from the end of a #2 pencil to the size of the last section on my index finger. Their firmness was like that of a ripe orange. They were not squishy nor were they bead-like in firmness.
Stoney sneezed much more when these bumps invaded her muzzle. The bumps were not visible to me in the muzzle but were found on necropsy. They inhibited airflow causing labored air intake and thick mucous discharge from her nose.
Feeding Stoney became difficult. As with many cancer patients, what seemed appetizing one moment was not the next. Like most owners with Berners with cancer we tried everything we could think of including raw meat, cooked meat, peanut butter, cookies, broths of various kinds and just about anything in the house. Some days she ate very little. Other days her appetite was pretty good. The disease process seemed to wax and wane during a "cycle" with a steady progression of symptom advancement from cycle to cycle.
Dr. Moore had a theory at the time regarding the stage of development of the thymus gland and the onset of histiocytosis in Bernese. Stoney was the youngest reported case so far and he wanted, on necropsy, to discern if she had yet lost her thymus gland as dogs do as they mature. All the other cases were in dogs old enough to have lost their thymus gland. With his theory in mind, Stoney was used in an experiment in which I injected her weekly with freeze-dried calf thymus supplied by Dr. Moore.
Stoney was euthanized at 22 months, about 13 months from onset of symptoms and 7 months following her diagnosis. Necropsy revealed her thymus gland intact and systemic histiocytosis.
Malignant Histiocytic Sarcoma
Jennie Lanseigne-Hoffnagle � Tully, 2/17/93 � 12/8/99
Tully had his right anterior cruciate ligament repaired in January 1997. The surgery appeared to be successful for about a year. Within a span of 2 years, he had 6 surgical procedures on his right knee joint, as well as an ACL surgery on his left knee in September 1999. The exploratory surgeries on his right stifle did not show evidence of cancer until an orthopedic surgeon suspected that he found abnormal tissue within his stifle in March 1999. The biopsy of that sample was confirmed to be Malignant Histiocytosis Sarcoma by three pathologists in three different laboratories. His bloodwork was always within normal ranges, and radiographs of his abdomen and chest were always clear of the cancer. A bone marrow aspirate and a lymph node biopsy of the popliteal lymph node behind his knee were both negative for any abnormal cells. We were prepared to amputate his right leg to prevent the cancer from spreading, but he tore his left ACL just days before the scheduled surgery. Since he was still symptom free, and a very happy, content dog, we made the difficult decision to correct the injury to the left cruciate ligament. His recovery from that ACL surgery was remarkable because he could not use either of his legs for several days. The strength of his left hind leg was tremendous, and he healed very quickly. Tully lost weight slowly at first, and the only sign that he was ill was his chronic limp from the invasive surgeries throughout the years. We treated Tully with traditional and holistic therapies. Acupuncture, regular RIFE treatments (a method of using vibrational energy for healing discovered by Royal Rife, see http://www.naturesalternative.com/rife.html), anti-inflammatory medications and holistic remedies, as well as a modified diet were the methods that we chose to help him feel happy and comfortable. Tully's weight had dropped from 108 pounds to 96 pounds gradually over the last few months of his life. On the morning of December 8, 1999, he showed no interest in his food, was depressed, had labored breathing and started vomiting. Chest radiographs still showed no evidence of the cancer invading his lungs, but it was then that we decided that he was fighting a losing battle. We euthanized Tully at the age of 6 years 10 months old.
Amanda Harvey � Griffon: 12/18/97 � 11/11/02
Griffon was an avid swimmer; he would spend all day in the water, barely coming out for a breather. But by the beginning of July, he would leave the dock and go lay on the patio by himself after swimming only for a bit. At the time, we thought he was trying to avoid getting a bath. Looking back- we know that was the beginning. About a month later, Griffon then started to lag during walks when before he would be out front, pulling away. We noticed he was doing it all of the time, not just on occasion. We also noticed he had lost a lot of weight. He usually dropped weight over the summer from swimming so much, but this was not normal- I could feel his ribs.
The first week of September, he started to turn down food- I called the vet. The local vet did blood tests which showed Griff's proteins were very low, as was his red blood cell count. They did X-rays but couldn't really see anything. They did an ultra sound the next day at which time they saw his spleen was enlarged, and they took some aspirates from his spleen & liver. At this point we knew something was seriously wrong with him so we went to The Veterinary Hospital at the University of Pennsylvania (VHUP).
VHUP vets did a physical exam and ran some tests. They confirmed that Griffon's spleen was "huge". They referred us to an oncologist, Dr. Clifford. Griffon was diagnosed with Malignant Hystiocytosis Sarcoma when all of his test results came back at VHUP. Clifford had a colleague who had some success with a new chemo drug, Lumestein. VHUP was doing a study and wanted to give Griffon an MRI (which we wanted to do anyway). So Griffy had the MRI, which showed more clearly that his spleen was indeed severely enlarged. The aspirates showed some cells were in his liver as well, but Griffon was in the beginning stages. At this time I asked if removing his spleen was an option- Dr. Clifford said no since Griff did have some cells in his liver.
Griffon started Prednisone which gave him his appetite and bounce back. The vet also prescribed 300 mg/per day of Omega 3 Fatty Acid. He got his 1st round of chemo- 3 pills given orally. He was acting pretty much like himself. He took a few more naps throughout the day, but he was happy. Griffon's eating habits became fickle- he rarely ate dog food. He started out only eating filet, then moved to chicken. Then we discovered he loved chicken livers so we added that to his diet. Griff went from 79 lbs back up to the low 90's. He was begging for food again, wanted to go for his walks, etc. The chemo didn't have too much of an affect on him as far as side effects. He was doing very well. With the chemo, he had to get blood tests every week to check his platelet count. The chemo was a balancing act- keeping all of the levels in check. The chemo is given every three weeks.
After his initial dose, Griff had blood work a week later to see where his counts were. After receiving the blood work, VHUP called to see how Griffon was. Apparently his counts were really low and they assumed he was hospitalized. I told the vet he was doing fine- no change in behavior at all. She prescribed an antibiotic just to be on the safe side and said to watch him for any changes. After his next blood test, his platelet count had risen significantly. At Griffon's next chemo visit to VHUP they found that his spleen had shrunk by 25%. But Griffon's blood counts were lower than what the vet would like in order to administer the chemo. Giving him the chemo could cause his platelet count to crash even more, which could cause internal bleeding. He said since there was no protocol with this treatment, he couldn't tell us what to do. It was up to us as to whether Griffon got the pills or not. We consulted with a friend who is a MD. He said if we were going to treat the cancer, we had to treat the cancer- no matter what. We gave Griffon the pills. He didn't crash.
Griff continued to do well for the next 3 weeks. When he returned to VHUP for his 3rd round of chemo, his platelet count was all the way down to 4,000 (it should be in the 100,000's). He couldn't get the chemo. He was to return in a week to see how he was doing. VHUP sent us home with Sulcrate and Pepsid to coat Griffon's stomach as a precautionary measure against internal bleeding. The next day, Griffon stopped eating. We tried all of his favorites, but he was only taking a bite here and there. The vet suggested baby food. Mild-mannered as always, Griffy let us put the baby food in his mouth, and he swallowed it. His energy diminished greatly. He started to get sick- he threw up a few times and had diarrhea. The diarrhea continued until Friday. The vet said it could possibly be the chemo catching up with him since the toxins have a cumulative effect. We gave him anti-nausea pills, but his appetite never returned. Griffy didn't move much over the weekend. He appeared to be uncomfortable, constantly shifting to find a comfortable position.
We knew we had to make a decision since he wasn't getting any better. His health has been deteriorating for a week and he didn't show signs of improving. That Monday Griff didn't move at all- he just laid there while everyone pet him. We noticed his back legs were extremely swollen- they were filled with fluid. We later found out this edema is caused by the proteins not being delivered to the correct places, so the cell break and release fluid- this would have continued throughout his whole body. From the day we found out Griffon was sick, we swore he would not suffer. We put Griffon to sleep that night. I truly believe the chemo gave us an extra 6 weeks with Griffon we would not have had otherwise. And we treasured every second of it.
[Note: Chemo was around $65 for pills, $35 for office visit. That was every 3 weeks. Plus - blood tests every week, which was about $75. VHUP paid for the MRI.]
Malignant Histiocytosis
Pat Long � Hannibal, 7/29/88 � 5/23/93
Hannibal was 4.75 years old when he walked away from some food in his dish one day. I knew there was trouble, but thought it was a sore tooth. He had swollen lymph nodes under his front legs, and when the vet couldn't find anything wrong, he did a full blood workup. Hannibal's appetite stopped entirely within a week of the first sign of trouble, and even prednisone wasn't stimulating it. When the liver enzymes came back 4 times normal levels, we had an ultrasound done. Multiple lesions found in both liver and spleen. I allowed myself to be talked into letting them biopsy the tumors, but he didn't live long enough to get the results. Weak from lack of food, jaundiced, his urine dark brown, he was euthanized two days later. I had him only three weeks from the time he first turned away from any food, but I was lucky - many get much less than that. Pathology results found tumors in the liver, spleen, lymph nodes, lungs, and left hip joint capsule, diagnosis malignant histiocytosis.
Alison Jaskiewicz � Jay Jay, 4/20/89 � 8/16/97
In July 1997 alone Jay Jay and I walked almost 50 miles in our New Hampshire woods together. Jay Jay leaped and bounded, chased squirrels and chipmunks, flopped in mud puddles and howled his beautiful songs for me � the picture of glowing health. On August 12 our world crashed in on us. We went out for our early morning walk with Jay Jay bouncing and dashing about as usual. As he dashed back to check in with me, tongue lolling out the side of his mouth, I saw he had no color in his tongue or any of his mucous membranes. End of walk, called the vet and took him in. Nothing obviously wrong except his pallor. Took blood for analysis. Vet called next day to tell me his platelet count was so low he could spontaneously hemorrhage at any time. On August 14 we went to Tufts where I left Jay Jay (still happy and bouncy) for further tests. Abdominal x-rays showed an enlarged liver so an ultrasound and needle biopsy were scheduled for Friday August 15. The call and diagnosis devastated us � malignant histiocytosis. We knew this was a death sentence. We opted for low level chemotherapy treatment to help him be more comfortable in the ensuing 4 - 6 weeks we thought we had. We visited Jay Jay that night. He greeted us with happy wags but during our hourlong visit he was tired and wanted to sleep, relaxing against us on the floor as we stroked all his favorite places. We left promising to visit the next day but that was not to be. After a comfortable night according to the vets and staff, his body just shut down. Jay Jay died about 9 the next morning. I still have a hard time with the fact that I was not with him at the end. Postmortem liver samples sent to UC Davis confirmed the malignant histiocytosis diagnosis. Bottom line, we went from an apparently healthy dog to a dead dog in four days and we lost him 17 hours after we received the diagnosis. Jay Jay was on a homemade all natural diet his entire life with us - from 5 months on.
Sharon Gaffney � Crystal, 02/02/94 � 06/05/00
Crystal started doing poorly, at three years old she was losing weight rapidly. X-rays revealed a corncob stuck in her intestines, but it also showed a slightly enlarged spleen. After consultation, the vet decided to remove both the corncob and the spleen. Pathology showed minute amounts of histiocytic cells in the spleen. It wasn't until three years later that Crystal began to fail, and in four weeks from start to finish Crystal went from being a bouncy healthy girl to dying of malignant histiocytosis. Necropsy revealed tumors in her lymph nodes, lungs and surrounding the heart. We feel very lucky to have had her as long as we did; If she didn't raid the trash when she was three, we may have lost her much sooner!
Elizabeth Malcolmson � Tycho, 03/25/90 � 10/15/98
October 2nd, coming home from our morning walk, I noticed Tycho's leg was terribly swollen. Finally, something more we can point out to the vet. She had lost a lot of mass and had acted "not herself" which the vet had attributed to an overall system drain after a very bad hotspot. The swollen leg and a rash across her abdomen worried the vet considerably. X-ray showed a large mass on her spleen, and an enlarged lymph node on the base of the spine. Her platelets and blood proteins were low and she was anemic. The rash was evidence of surface hemorraging. Rushed to Tufts, and were told that it was either malignant histiocytosis, or something else just as bad. They had things they try, but nothing that works. They wanted to admit her where they could administer fluids and, monitor her condition, and do some tests, but quite possibly the tests could kill her. We opted to take her home with us and when she came bouncing out to see us and demanded a cookie from their front desk, it was clearly the right thing to do -- even that moment of joy might never have been experienced. She panted a lot, but the prednisone as well as her thyroid medication could cause that. We stopped the thyroid meds. She insisted on being outside a lot, but was very happy to greet family and visiting friends. She refused to eat any "normal food" but enjoyed Harriet Gehorsam's Magic Meatballs and up to the last weekend would demand things like pancakes sitting on the counter. During our last two weeks, she would make extra surprise trips upstairs when she really didn't have the energy, to be with us. She would get up on the couch and demand to be petted when she didn't have the ability to do the stairs any more. She needed help to get into a standing position and once, after getting me out of bed to help her stand, took the opportunity to get into my place in the bed!
Within two weeks, her packed cell volume fell to 17, which was "incompatible with life" according to the vet. In the next day, it was clear that her energy was a non-renewable resource. On the last morning, she lost control of her bowels and had no strength. The night before she had finally been able to sleep, something she hadn't really done in weeks. It was clearly time for her to go.
Pathology results showed anaplastic histiocytic cells in the spleen, and the pelvic lymph node. The Berner-L family held our hands and were an enormous support as we made this first-time journey. As awful as the experience was, it convinced me of the true nature of heaven -- a place where Tycho would be restored to us in perfect health and utter happiness.
Susan Ablon � Wendy, 10/87 � 4/94
My first experience with malignant histiocytosis came in 1994, shortly after the birth of my first litter by six year old Wendy. She was a healthy sound (excellent hips and one of the first OFA elbows #6) good natured dog. She was a natural whelper and a great mother. There was no medical problems with this dog that I could see. Sadly 6mos after the whelping of this one and only litter my girl developed a slight cough. She was still very active, her appetite was good and we treated her for what seemed a slight kennel cough. Sadly, this cough worsened and further exam showed that both lungs were whited out (congested). When she did not respond to anti-biotics we began to look at possible cardiac problems none of which could be found. Over the next few weeks her breathing became more labored and the only suggestion my vet had left was to do a tracheal wash. I refused since IMO (and that of my vet) it was very possible that this would be enough to kill my dog. Rather I spent the last night holding this sweet dog in my lap and the following morning sent her over the bridge. Necropsy showed widespread cancer throughout the lungs, liver, and spleen and the biopsy came back malignant histiocytosis.
The sad thing to this story is that the hereditary component of malignant histio was reported by Dr. Padgett at the specialty the month after Wendy's death. I was devastated that my first litter was now at risk. As a breeder it's not as if I haven't suffered for the loss of a very wonderful dog that I owned and bred but feel the loss of each of the dogs that I produced and the suffering that the families that owned these dogs have gone through. When they called or I heard of the illness there was nothing I could do to help them or encourage them. There is no treatment, there is no advice I can give. This is a devastating cancer and we have no answers to treat it effectively at this time.
I knew that histio was a problem within this line. I knew that Wendy's grandmother died of histio (reported by the owner) at 11 years old. Wendy's mother died of histio (reported by the owner) at 8yrs. I also knew that some of the dogs in this line lived to 9,10 and 11 years so felt that if Wendy were bred to a dog with longevity things would be ok. I'm not so sure now if I would have done the same breeding today. I did choose a stud that had longevity behind him - father and uncle lived to 11, mother lived to 13 and other dogs showed a variety of ages and causes of death. To date I am aware of one of Wendy's offspring dying at 5 of what sounds strongly like histio and another confirmed at 7. Two offspring are still well at nearly 8 years and one died as a pup by being hit by a car and one is unknown. No further breedings came from this pedigree.
Karen Connors � Britney, 05/05/93 � 7/1/99
Britney started going off her food in January. Shortly after, when she was lying down and I was rubbing her belly, I found a lump I knew should not be there. I took her in for an ultrasound and the vet knew immediately that her spleen was enlarged. She had the spleen removed and it was engorged with Malignant Histiocytosis. I treated her holistically (using Marina Zacharias, www.naturalrearing.com, email - ambrican@cdsnet.net) and traditionally. She acquired a lung infection that we were not able to eliminate. The vet used the antibiotic Baytril to keep the infection under control. She finally stopped eating, and refused all of the supplements, the Baytril stopped working as well. Britney died July 1st, almost one month past her sixth birthday.
Catherine Cairns � Max, 7/23/90 � 8/2/00
Max was almost 10 when I noticed that he was less keen on food than usual. He had always had a good appetite, so this was a cause for concern when it persisted beyond a day or two. It was winter, so not related to hot days or any other easy explanation.
We went away for the next weekend and took the dogs to a beach house with wooden floors. Max appeared to have some trouble negotiating the floors, but I put this down to unfamiliarity. One night he could not settle and would occasionally yelp in pain for no apparent cause. He had run around that day far more than normal in the excitement of being at the beach, so I thought he may have aggravated his arthritis, and tried to keep him calm.
When we returned home, I watched him and took him to the vet on the Wednesday. The vet thought it could have been arthritic pain and gave him a shot which I was advised would work within 24 hours. I was advised to take him back if he did not improve. He seemed to pick up and ate a little, so it was not until a week later that I felt something was not right, and his appetite had worsened again. I took a urine sample to the vet which was dark orange in colour. His gums were very pale. The local vet xrayed his chest, which was clear, then recommended an abdominal xray. This showed shadowing which the vet felt may indicate neoplasia (cancer) of some sort. The blood showed high levels of white cells and protein in the urine. He recommended ultrasound at a vet hospital, which we had performed the same day. This showed multiple lesions in the spleen and pancreas, and a small bleed into the abdomen. Max was having difficulty rising at the vet hospital.
He was euthanised the same day. Necropsy confirmed malignant histiocytosis, with marked jaundice of body tissues, fluid in the lungs, abdominal and thoracic cavities. There was marked enlargement of the liver, tumours on the liver, pancreas and spleen, and involvement of lymph nodes. The heart was affected. The case was unusual, having no involvement of the lungs.
We were blessed with him for 10 years.
Christy Kabler � Blithe, 4/16/95 � 1/25/00
Initially, the only indication that anything was wrong with four year old Blithe was a change in appetite and bad breath. She still showed an interest in food, but would only eat smaller portions more frequently. Written off by the vet as a dislike for her food, a change in food made no difference as Blithe gradually lost weight.
Then in December I heard her cough three times one morning. Blood work showed her packed cell volume (PCV) was 36 which was low normal. A test from the prior year showed a PCV in the mid 50's, so she was given supplements for anemia. Briefly she showed new symptoms � occasional limping (similar to polyarthritis) and corncob chewing at her legs � but these cleared up, perhaps due to the imuno-suppressive drugs she was given. The vet suspected pancreatitis because of the enlarged spleen, but her PCV continued to drop.
One Coomb's test was negative, the second was positive, so she was assumed to have auto-immune hemolytic anemia. Subsequently, she was diagnosed with Evan's Syndrome, an immune mediated anemia and thrombocytopenia. The vets were unable to determine the cause of the weight loss or to bring the continued drop in the PCV under control. A food tube was put in so that she could be fed through the tube if she continued to refuse food. Our fear was that she would starve before we could diagnose and treat the disease. Drugs, transfusions, none worked. A bone marrow extract showed contradictory results, one part showed a cell eating process called hemophagicitis that can occur in malignant histiocytosis, and the other part of the marrow showed no such symptoms.
When Blithe's PCV dropped to 9 she was euthanized. Unable to stand for long on her own, she was still alert and happy. Her sweet nature never failed. A necropsy was done but the initial lab was unable to make a definitive diagnosis. Not until the samples were sent to the lab at UC Davis could we get a firm diagnosis � Blithe had malignant histiocytosis.
I would urge all breeders to encourage puppy owners to perform necropsies in the event that they lose their dog to an undiagnosed illness. And I would like to thank a wonderful vet who never stopped trying to help, Blithe's very supportive breeder, and many others who were emotionally supportive.
Took Visuditibhan � Devon, 11/13/92 � 9/18/98
June 23, 1998, we took Devon to see our vet because we noticed that, recently and on several occasions, Devon had coughed (once or twice) while he was sleeping. Otherwise, he was healthy, active, and happy, and always had a good appetite. The chest x-ray showed a tumor in the lung. Subsequent examination by an oncologist revealed two nodules in the spleen and a mass in the abdomen. The lab results of samples taken via needle aspiration were diagnosed to be Malignant Histiocytosis.
Devon received two treatments of chemotherapy (Doxorubicin-based protocol) with a three week interval. We did not expect a miracle but hoped to delay the tumor growth. Further decision for additional chemotherapy session would depend on the results of these two initial sessions. Devon also had weekly acupuncture to help boost his energy.
During the course of the chemotherapy treatment, Devon began to have less of an appetite but was still happy and eager to go for his daily walks. We switched to home-cooked diet and gave him Vitamins C, E, B complex and other supplements.
Several days before we were due back for the follow-up check on the second chemotherapy, Devon became weak in his rear to the point that he could no longer stand or support himself. He crossed the bridge on Friday, September 18. Our vet's final entry in Devon's medical record was, "multiple tumors located in both chest and abdominal cavities, 8 masses in lungs ranging in size from 1 cm to 10 cm diameter, over 10 nodules in liver, 3 in spleen, mesenteric ln grossly normal, as were stomach, intestines, kidneys."
Nancy and Linda Bates, Xena, 9/28/95- 5/9/00
We lost, Xena, our precious 4 1/2 year old Berner girl, to histocytic sarcoma in May of 2000.
Xena had an uncommon form of histiocytic sarcoma that is associated with hypersplenism, anemia, and prominent splenic hematopoiesis (red blood cells being made in the spleen). The splenic phagocytes (both the cancerous cells and the "normal" cells) are increased in number and activity and they destroy the red blood cells, causing anemia.
Because Xena's symptoms (anemia, loss of appetite, enlarged spleen) presented differently than "classic" malignant histiocytosis she was misdiagnosed by our local vet and the vets at a major Boston animal hospital as having immune-mediated hemolytic anemia (IMHA). Her vets didn't think that removing her spleen was the best course of action so the surgery was delayed until March. About 3 weeks after sending spleen samples to UC Davis, Dr. Moore gave us the true diagnosis. The type of histocytosis that Xena had is rapidly progressive (1-5 months) and there is often concurrent involvement of the bone marrow.
Xena led an active life and she earned numerous draft and agility titles. Since she LOVED to eat, we were very concerned in early February of 2000, when she began to get picky about her food. At first Xena didn't want to eat her veggies. Then she didn't seem to want the kibble.
We took her to the vet and they said she was fine. A few days later Xena's abdomen felt taut and her gums seemed pale. Palpation and X-rays indicated an enlarged spleen. Moderate numbers of spherocytes were noted on the blood smear, indicating immune-mediated hemolysis.
Her ultrasound showed a 3 cm x 2.8 cm diameter cavitated area on her spleen. There was also a cyst on her liver but the vet did not think it was related to her illness.
Our primary vet felt strongly that Xena had IMHA and that we'd lose her if we didn't start her on prednisone. The upside of the prednisone was a huge improvement in her appetite and the "swelling" of her spleen dissipated. However, her gums were very pale and she had several episodes of high heart rate and panting. These "episodes" which were side effects of the prednisone tended to happen when she was resting, around 5 AM, and after she ate.
Xena's spleen biopsy showed that she was making red blood cells in her spleen (which is abnormal in postnatal life). The ultrasound technician did not biopsy the 1.5 cm cyst on the spleen because she thought it was a hematoma. The bone marrow smears suggested that Xena's anemia was due to accelerated destruction rather than diminished production and were supportive of the clinical suspicion of IMHA.
Xena seemed to be improving since the prednisone was increased to 60 mg/ day but even though she was eating anything and everything she lost nearly 6 pounds in 2 weeks. Her PCV was still low at 23.
We had a bionutritional analysis done by a holistic vet, Dr. Konrad Kruesi, and we started Xena on thyroid support, Visioplex, Vasedex, Lecithin, Gynplex, and Ferrofood to facilitate the production of new red blood cells, enhance immune function and stimulate her liver to be active again. The analysis showed that Xena also had a glucose-6-phosphate deficiency so we had a compound made up by Pet Health Pharmacy to address that deficiency. We switched Xena from prednisone to natural cortisol to reduce the side effects of the steroids.
By the end of February, the specialists started to reconsider the IMHA diagnosis.
On 3/8/00 Xena's primary vet removed her spleen. There were pale patches of "necrosis" in her spleen. Her liver was slightly enlarged. Her PCV was 20.
The pathology report that we got back from Cornell didn't give a clear diagnosis, so we sent spleen samples to Dr. Moore at UC Davis. On 3/29/00 we got the diagnosis back: "Histiocytic sarcoma, multiple sites, spleen. This lesion is not easily treated and progression is anticipated. Your dog will likely experience metastatic disease soon - first to the liver and then the lung. Progression can be variable but is usually fairly rapid (just a few months)." Dr. Moore didn't find any evidence of histiocytosis in the bone marrow sample that we sent.
Xena's PCV began to drop. She had 10 blood transfusions between 3/17 and 5/9. Her PCV dropped from 17 to 9 during that time.
Xena's gums were very pale and she was very picky about eating, taking food only if she was hand fed. It was difficult to get her take all the supplements (about 50 pills a day plus poly MVA). She was exhausted all the time.
None of the medical schools in MA had anything to offer us so we did a phone consult with Dr. Loops, a homeopathic cancer specialist. The remedies he prescribed (phosphorus, china) were the only "drugs" that seemed to help her feel a bit better.
We took her to Marty Goldstein's clinic in NY and he took the case on himself. He gave Xena packed cells, ozone therapy and every other treatment he could think of. He sent her home with immuno-augmentative therapy (IAT) that involved giving her subcutaneous injections several times a day. He also started her on an anti-cancer drug, Ukrain, that we imported from Europe. Since the Ukrain required intravenous injections, our local vet continued the Ukrain treatments. Xena had about 6 Ukrain treatments. She lost all interest in food after the injections and had diarrhea (which is supposed to be a side effect of ridding the body of toxins). We also gave her Epogen hoping that it would boost her red cell production.
Xena endured all her treatments willingly. She wanted to stay with us as much as we wanted to save her. It could have been a coincidence but every time we tried to add an anti-cancer treatment (Ukrain, cloud mushroom extract, red clover hoxey, etc...) her PCV seemed to drop more quickly.
By 5/3 the transfusions were only lasting a day. On the night of 5/8, Xena was having trouble breathing. We took her to the local emergency vet. Since they didn't have blood available they transfused her with oxyglobin. Her breathing was still labored when we got her home. Her liver was enlarging and we just couldn't bear to make her suffer any longer. We put her down on May 9, 2000. She went to sleep in our arms hearing how much we love her. She was truly our strong, brave warrior princess.
Xena had a history of autoimmune reactions and the coccidia and urinary tract infections she had as a pup may have been an indication of immune dysfunction. When she had her last rabies and distemper shots in 1996, she went into anaphylactic shock and had to be revived. Since Xena had high titers, we never vaccinated her again.
Both of her parents died at age 5 and her sister died of "bone cancer" shortly after Xena's death. MH is an inherited disease and it is horrible the way these dogs suffer. Please do anything you can to support the research being done by Dr. Moore at UC Davis.
Our advice is to raise you dogs holistically and treasure them every minute of every day. We shared a lifetime of adventure with Xena in the 4 1/2 short years that she graced our lives. Her beautiful, loving spirit will always be guiding us.
I did find a matrix metalloproteinase inhibitor (col-3) that is supposed to be able to cause programmed cell death in a human histiocytic lymphoma cell line. Histiocytes produce matrix metalloproteinases that degrade cell tissues. That's one of the reasons that this cancer can spread so quickly. The product, made by CollaGenex Pharmaceuticals, was only in phase 1 clinical trials so we couldn't get it. Col-3 is the only drug I found that claimed to be effective against malignant histiocytes.
Donna Soderstrom � Baci, 10/10/96 � present, 9/6/2005
"Baci" Kiss of Frost v Bev's CD JHD CGC - On March 2, 2005 Baci had a TPLO to repair a ruptured ACL. When the orthopedist called after the surgery he said there was some abnormal tissue on her femur. He had sent it out to a lab. A week later we heard from Indexx Labs in Texas. The pathologist suspected histiocytic sarcoma. He was sending the specimen back to my veterinarian, Dr. O'Brien, to be forwarded to Dr. Moore at UC Davis.
It was towards the latter part of the month when we heard the confirming diagnosis. It was a histiocytic sarcoma. I was anxious to know what treatment options might be available. At this time Baci was lively, and appeared healthy. I began gathering information on my own while we waited to hear about treatment options. The first message regarding treatment only offered amputation of the leg. Baci has bad elbows, so I had already ruled that out. A week later we were advised that radiation might be an option. On April 18 we received a call telling us we would be seen on April 25 for staging. If Baci's cancer had spread, there would be no point in doing radiation. I was told at this time that there was no chemotherapy available.
I have learned that Dr. Moore's lab is separate from the Veterinary Teaching Hospital. I should have had my veterinarian call for a staging and evaluation the moment we had confirmation from Dr. Moore. A lot of dogs don't have seven weeks to wait.
They called it staging, but they don't really stage this disease. If it has not spread it is histiocytic sarcoma. If it has, the name is changed and it is malignant histiocytosis (MH). That afternoon we received more bad news. It had spread, she had MH and there was no point in doing radiation. Her lymph nodes, spleen and lungs were affected. But then I was surprised. They asked if I would like to try chemo for her. They were just seeing some results from a small study from the University of Pennsylvania. The goal would be to slow the progress of the disease and maintain good quality of life. The drug they were using is Lomustine, otherwise called CCNU. It is can be toxic to the liver. We would watch her liver enzymes closely. This is an oral medicine and treatment could be given through the hometown vet. Side effects could include nausea, diarrhea, lethargy and fever. They would be most likely at the peak period of the drug, in the 7-10 day period after her pills. I decided to give it a try. She seemed so healthy that I felt she had the reserves to tackle this.
Baci had been on the Colorado State cancer diet since November (when Oso had been diagnosed with his disease). It is essentially doggie Adkins: low carbs, raw, pureed cruciferous vegetables, meat (cooked turkey), bone meal, vitamins, supplemental oils, particularly Omega 3. Extra selenium to fight the cancer. Milk thistle and vitamin E for the liver support. I have been using artemisinin, an herb found in Vietnam, which has shown some promise in reducing tumors. The oncologist, conventional vet and holistic vet have all been consulted and informed about everything I'm using on her. One must be careful here, for example artemisinin should not be used in conjunction with radiation therapy.
As predicted she had fever, diarrhea and lethargy lasting about 36 hours about a week after her treatment. Then she bounced back to pretty normal. On our second visit tests showed her liver enzymes were rising. I had just read something about SAM-e and asked if that might help her liver. Our oncologist, Dr. Romansik, agreed that it might help, and we delayed chemo for a week to let the enzymes come down. A week later the results were good enough to continue. I firmly believe that the SAM-e, along with the milk thistle and vitamin E, is essential to combating the toxicity of the CCNU. Dr. O'Brien followed up with information from a colleague at Cornell with a lot of data to support SAM-e's role in liver support. Baci's chemo regime was changed to every four weeks instead of three, with 70 mg. of CCNU instead of 90mg. It became apparent to me that Baci would benefit from having all tests and treatments at Davis. It has allowed us to do follow-up tests as needed to provide the clearest picture of her health. With the longer interval and lowered dosage her side effects were minimal - one day of loose stool. That's it.
Treatment four. Tests were showing a reduction in her lymph nodes, and spleen. A chest X ray showed the lungs were at least stable. We scheduled treatment five. No dog, to Dr. Romansik's knowledge, has made it to treatment five.
Treatment five. August 21, 2005. The x-rays show that her nodules in her lungs are clearly reducing. Liver values are down at normal levels. All blood work is good. She is a happy girl. She looks wonderful. Her weight is stable, appetite excellent, her coat is lovely. We have been using 15 mg. of prednisone every other day to reduce the discomfort in her leg. I worry about the bone being brittle, especially because she feels so well and can be wild.
We still take every day one at a time. We are, as Dr Romansik says, in unchartered territory. I am awfully glad to be here! She is six months post diagnosis. We have chemo number six planned for September 21, 2005
Costs: The initial appointment at Davis was about $700.00. Each visit runs $200.00 - $300.00; it varies with the tests done. I take the whole day off work to give them time to do what they need. I am spending a lot on the supplements she takes, too. (Thank God for Costco!)
A Teaching Hospital � It can be bureaucratic. I have had more than enough small snafus, almost at every visit. But the high quality of medical care more than makes up for this. I am very happy with Baci's oncologist. I feel he's really fighting this with us.
I do not wish to give anyone false hopes with our story. But she is doing better than we had ever hoped. One additional thing is that Baci is a confident, gregarious dog. She is not stressed by going to Davis. I would encourage anyone facing MH with his or her dog to try to keep your options open to both holistic and traditional treatments. It is only when we are willing to take a chance that we will come upon a cure for this.
Not Histio, but important lessons
Pat Long, Maggie - 3/21/92 - 7/17/01 � NOT histio
Maggie was 9.5 years old, and started appearing to gain weight. It took a week to realize that she wasn't gaining normal weight, but her abdomen was becoming enlarged, probably from fluid. X-rays showed an enlarged liver, and both my vet and I knew what that meant. It was less than a week that she stopped eating, and within another day or two she weakened to the point that I could no longer allow her to suffer. My vet and I were sure that it was histio.
He did the necropsy, and I had him send samples to his normal area lab as well as to UC Davis. Maggie's liver was over 75% tumor, and smaller tumors were spread throughout her abdominal cavity, covering her other organs. The area lab was unable to make any determination as to the type of cancer - the liver cells were so diseased. My vet had them cut a fresh sample and retry, but the results were the same. He and I both were still sure of what it was we were dealing with, after all, she was a Berner.
The report came back from UC Davis - hepatocellular carcinoma. This is basically liver cancer, it is not specific to any breed, does not seem to be hereditary, and when it strikes, it is usually older dogs, aged 10 - 12 or so.
My conclusions? This is a perfect example of the real need for careful and accurate diagnosis of cause of death. Had we gone with the obvious assumption, Maggie would have been listed in Berner-Garde as presumed to have died of histio - and who would have thought it wrong? But any studies or review of family data would have been inaccurate because of that inaccurate assumption.
Ruth Reynolds, Promise � 3/88 � 12/97
Hope's Pioneer's Promise was born in Pioneer Bernese's first litter. She was traded as a puppy to Julie Steinheimer of Hope's Kennel and was purchased by us when she was about two years old.
Promise whelped four litters here and was spayed at age eight due to a continuous discharge odor which was troublesome to our males. Her ovaries and uterus looked completely normal but sections were sent for histopathology anyway. Results showed adenocarcinoma in the ovaries. I didn't expect to have Promise with us much longer.
Following the spay, Promise gained some weight and seemed to do very well for about a year. Then she became a bit more picky about her what food she wanted to eat and she dropped some weight. With declining condition, at 9.5 years she was euthanized and a necropsy performed.
In the necropsy my vet took samples from all major organs. I suggested we excise a bump in her skin that had a slightly scaley surface of hair loss.
Necropsy results: adenocarcinoma involvement in her major organs and systemic histiocytosis in the skin sample. Her mother had succumbed to the ravages of malignant histiocytosis at ten years of age.
Jean Cheeseman maintains a series of web pages presented in Loving Memory of Bernese Mountain Dogs
lost to Canine Malignant Histiocytosis. To see these pages visit "Histio Roll Call" at: http://www.angelfire.com/anime3/longlease/histiorollcall.htm.
 Histiocytic Diseases of the Bernese Mountain Dog
Histiocytic Diseases of the Bernese Mountain Dog